Vieussens’ ring
Vieussens’ ring
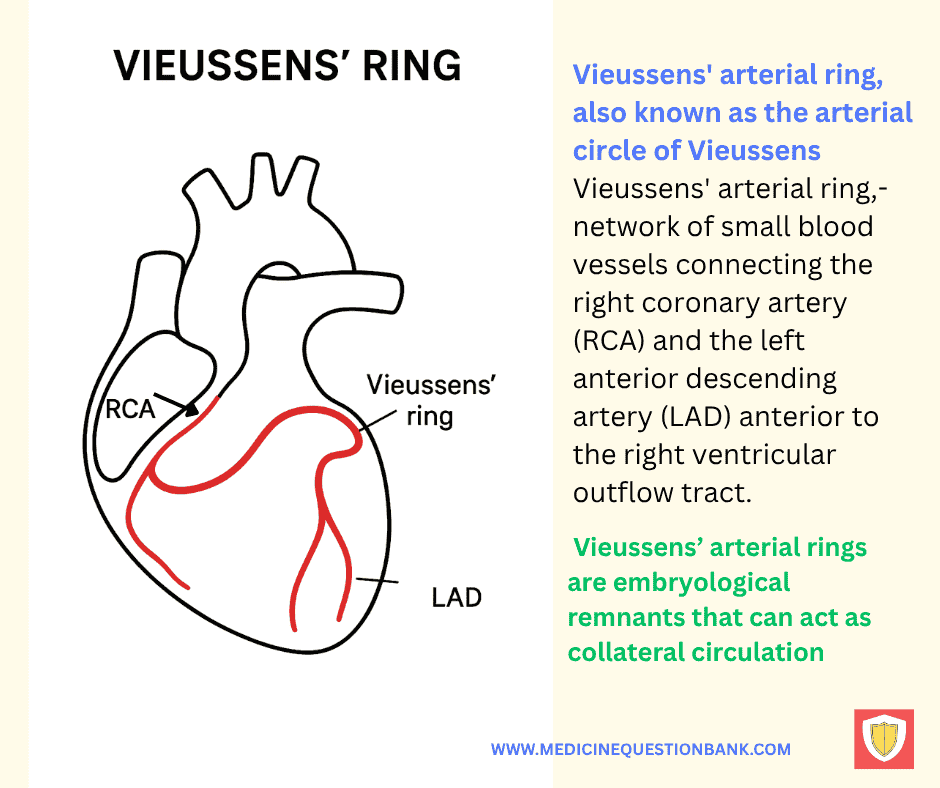
Vieussens’ ring is an important epicardial collateral arterial connection between the conus branch of the right coronary artery (or an independent conus artery from the aorta) and the proximal left anterior descending artery (LAD).
It forms a vascular “ring” around the right ventricular outflow tract (RVOT) and proximal interventricular groove.
Anatomy & variants
- Usually involves the conus artery → anastomosis → proximal LAD.
- The conus artery may arise from the RCA or directly from the aorta (anatomical variant).
- The ring can be single or multiple small anastomoses; size and prominence vary widely.
Physiologic / clinical significance
- Acts as a natural collateral pathway supplying the LAD territory when LAD flow is compromised (chronic total occlusion or severe stenosis).
- Important in coronary chronic total occlusion (CTO) — can maintain distal perfusion and influence symptoms, viability, and revascularization strategy.
- Can be a target for interventionalists when planning retrograde CTO PCI or assessing collateral circulation.
- Rarely, a prominent Vieussens’ ring may be involved with aneurysm formation or be confused with other vascular structures on imaging.
Imaging identification
- Coronary angiography: classic way to visualize — look for a vessel from the conus region crossing to the proximal LAD.
- CT coronary angiography (CTCA): shows course and calibre well; excellent for mapping variants and planing interventions.
- Intra-procedural angiograms: can demonstrate flow direction and usefulness of the collateral during ballooning or occlusion tests.
Interventional / surgical implications
- Presence of a well-developed Vieussens’ ring can:
- Mean better myocardial perfusion distal to LAD lesions (reducing ischemia).
- Provide a retrograde collateral channel that may be usable during CTO PCI (requires experienced operators).
- When performing bypass or ligation near the conus/RVOT region, surgeon awareness is useful to avoid compromising collateral flow.
- In some revascularization planning, collaterals may affect urgency/choice of revascularization.
Key pitfalls / pearls
- Don’t confuse a large conus-to-LAD collateral with an anomalous coronary artery origin — check ostial origins carefully.
- A prominent Vieussens’ ring may be the main blood supply downstream of an occluded LAD — occluding it (surgically or inadvertently) can provoke ischemia.
- Helpful predictor of myocardial viability distal to chronic LAD occlusions; presence argues for potentially salvageable myocardium.
One-line summary
Vieussens’ ring = conus (often RCA-origin) → collateral link to proximal LAD — an anatomically variable but clinically important collateral that can preserve LAD territory perfusion and influence coronary intervention strategy.
Vieussens’ Ring — 20-point Summary
| Topic | Detail |
|---|---|
| 1. Definition | Collateral connection between conus artery (RCA or aortic ostium) and proximal LAD. |
| 2. Origin | Conus from RCA or independent aortic ostium. |
| 3. Anatomy | Arcade around RVOT / proximal IV groove to proximal LAD. |
| 4. Variants | Single large vessel, multiple anastomoses, independent conus ostium. |
| 5. Role | Supplies distal LAD territory when proximal LAD compromised. |
| 6. Imaging | Best on selective angiography and CTCA. |
| 7. Perfusion | Can preserve viability distal to LAD occlusion. |
| 8. CTO PCI | Possible retrograde collateral channel (expert use). |
| 9. Surgical relevance | Avoid injuring conus collaterals during RVOT/adjoining repairs. |
| 10. Ostial ID | Confirm origins to differentiate from anomalous coronaries. |
| 11. Pitfall | Large collaterals may mimic anomalous arteries if not carefully assessed. |
| 12. Hemodynamics | Flow direction varies with pressure gradients (ante/retrograde). |
| 13. Complications | Collateral injury risks ischemia; retrograde PCI risks perforation. |
| 14. CTCA use | Pre-PCI anatomical mapping and planning. |
| 15. Perfusion correlation | Combine CTCA with SPECT/PET to confirm functional perfusion. |
| 16. Predictive value | Suggests salvageable myocardium distal to CTO. |
| 17. Interventional strategy | Influences retrograde vs antegrade approach and graft selection. |
| 18. Recognition | Look for conus→LAD crossing vessel on multiple angiographic views. |
| 19. Reporting | Document caliber, direction, and ostial origin in reports. |
| 20. Takeaway | Map and consider Vieussens’ ring in revascularization planning to avoid loss of supply. |
| No. | Question | Answer |
|---|---|---|
| 1 | What is Vieussens’ ring? | An arterial collateral loop connecting the conus branch of the RCA with the LAD. |
| 2 | Where is Vieussens’ ring located? | Around the right ventricular outflow tract (RVOT). |
| 3 | Who first described Vieussens’ ring? | Raymond de Vieussens, a French anatomist, in the 18th century. |
| 4 | What is the main clinical significance? | It provides collateral circulation in proximal LAD occlusion. |
| 5 | Which two arteries form Vieussens’ ring? | Conus branch of the RCA and proximal LAD. |
| 6 | How is it visualized on angiography? | As a collateral loop between RCA and LAD in selective injection. |
| 7 | In what percentage of people is Vieussens’ ring present? | Approximately 30–50%. |
| 8 | What is the alternate name for the conus branch? | Third coronary artery. |
| 9 | Why is it important in CABG surgery? | Preserving it can maintain myocardial perfusion during LAD grafting. |
| 10 | Which heart chamber does it encircle? | The right ventricle at its outflow tract. |
| 11 | What role does it play in acute MI? | May limit infarct size by providing collateral flow. |
| 12 | Is it more common in right or left dominant circulation? | No strong dominance correlation, but easier to see in right dominant hearts. |
| 13 | What imaging can detect it apart from angiography? | CT coronary angiography. |
| 14 | What is its embryological origin? | Persistence of anastomotic channels between early coronary buds. |
| 15 | Can it be a source of myocardial bridging? | Rarely, but the loop can run intramyocardially. |
| 16 | What does a well-developed ring suggest in chronic CAD? | Long-standing LAD stenosis with collateral recruitment. |
| 17 | Why is it sometimes called the “arterial ring of Vieussens”? | Because it forms a complete vascular loop. |
| 18 | What happens if both the RCA and LAD are proximally occluded? | The ring may be ineffective due to absence of inflow. |
| 19 | Is it considered an epicardial or endocardial vessel? | Epicardial. |
| 20 | Can it be used as a diagnostic sign for chronic ischemia? | Yes, its presence often indicates chronic LAD obstruction. |
Vieussens’ ring,,coronary collateral circulation,,right coronary artery to left coronary artery anastomosis,,conus branch of RCA,,LAD collateral pathway,, ,coronary artery collateral,,Vieussens’ arterial ring,,RCA conus branch anatomy,,collateral blood supply in coronary artery disease,,coronary bypass natural pathway,, ,anatomical pathway of Vieussens’ ring,,function of Vieussens’ arterial ring in CAD,,coronary collateral network anatomy,,clinical significance of Vieussens’ ring,,detection of Vieussens’ ring on angiography


