Right atrial (RA) pressure
Right atrial (RA) pressure
| IVC Diameter | Respiratory Variation | Estimated RA Pressure |
|---|---|---|
| ≤ 2.1 cm | > 50% collapse with inspiration | 3 mmHg (range 0–5 mmHg) |
| > 2.1 cm | < 50% collapse with inspiration | 15 mmHg (range 10–20 mmHg) |
| Intermediate findings | Variable collapse | 8 mmHg (range 5–10 mmHg) |
| Parameter | Criteria | Estimated RA Pressure | Clinical Notes |
|---|---|---|---|
| IVC diameter < 2.1 cm + > 50% collapse with sniff | Normal size, good collapse | 3 mmHg (range 0–5) | Suggests normal RA pressure and normal RAP waveform |
| IVC diameter > 2.1 cm + < 50% collapse | Dilated, poor collapse | 15 mmHg (range 10–20) | Suggests elevated RA pressure; check for RV dysfunction, pulmonary hypertension |
| Mixed pattern | Either small diameter + poor collapse OR large diameter + good collapse | 8 mmHg (range 5–10) | Intermediate category; consider other echo signs (hepatic vein flow, RA size) |
| Markedly dilated IVC, fixed diameter | No inspiratory collapse | 20 mmHg+ | Seen in tamponade, severe TR, constrictive pericarditis |
| IVC < 1.5 cm, collapses fully | Very compliant | 0–3 mmHg | Often seen in hypovolemia |
| Use in TR velocity–Bernoulli calculation | Add estimated RA pressure to RV–RA gradient | — | Essential for RVSP calculation |
| Alternative signs when IVC view not possible | Hepatic vein flow, RA area, right heart strain | Varies | Used when subcostal IVC imaging is suboptimal |
| Respiratory variation considerations | Assess collapse with sniff or quiet inspiration | — | Avoid deep exaggerated inspirations in patients with lung disease |
| No. | Key Point | Details |
|---|---|---|
| 1 | Purpose of RA Pressure Estimation | Helps assess right heart hemodynamics and estimate pulmonary artery systolic pressure (PASP). |
| 2 | Commonly Used Method | Based on Inferior Vena Cava (IVC) diameter and collapsibility with respiration. |
| 3 | Normal IVC Size | ≤ 2.1 cm in diameter. |
| 4 | Normal IVC Collapse | ≥ 50% collapse during a sniff indicates normal RA pressure. |
| 5 | Low RA Pressure | Typically 3 mmHg (range 0–5 mmHg) when IVC is normal in size and collapses > 50%. |
| 6 | Intermediate RA Pressure | Approximately 8 mmHg for intermediate findings. |
| 7 | High RA Pressure | 15 mmHg (range 10–20 mmHg) when IVC is dilated > 2.1 cm and collapses < 50%. |
| 8 | Severe RA Pressure Elevation | May exceed 20 mmHg in severe pulmonary hypertension or right heart failure. |
| 9 | Additional Clues | Hepatic vein flow reversal suggests elevated RA pressure. |
| 10 | Exercise or Stress Echo | RA pressure estimation can change dynamically with stress testing. |
| 11 | 2D vs. M-mode | 2D imaging preferred for accurate IVC measurement; M-mode may overestimate collapsibility. |
| 12 | Subcostal View | Preferred echocardiographic view for IVC assessment. |
| 13 | Technical Pitfalls | Poor subcostal windows, obesity, and mechanical ventilation can affect accuracy. |
| 14 | Effect of Mechanical Ventilation | Positive pressure can reduce IVC collapsibility and falsely elevate estimated RA pressure. |
| 15 | RVSP Calculation Link | RA pressure is added to TR jet gradient for right ventricular systolic pressure (RVSP). |
| 16 | Invasive Correlation | Right heart catheterization is the gold standard for RA pressure measurement. |
| 17 | Role in Heart Failure | Elevated RA pressure indicates systemic venous congestion in right heart failure. |
| 18 | Role in Pulmonary Hypertension | Helps in estimating pulmonary artery pressures and disease severity. |
| 19 | Serial Measurement | Useful for monitoring treatment response in heart failure or pulmonary hypertension. |
| 20 | ASE Guideline Reference | Based on American Society of Echocardiography recommendations for chamber quantification. |
1. Which echocardiographic parameter is most commonly used to estimate RA pressure?
Inferior vena cava diameter and its collapsibility
Tricuspid annular plane systolic excursion (TAPSE)
Right ventricular free wall thickness
Left atrial volume index
RA pressure estimation is most often based on IVC size and respiratory variation, according to ASE guidelines.
2. An IVC diameter ≤ 2.1 cm with >50% collapse on inspiration suggests an RA pressure of:
3 mmHg
8 mmHg
15 mmHg
20 mmHg
Small IVC with significant collapse suggests normal RA pressure, typically estimated as 3 mmHg.
3. Which echocardiographic window is most often used to measure IVC size for RA pressure estimation?
Apical four-chamber
Parasternal long-axis
Subcostal view
Parasternal short-axis
The subcostal view provides the best alignment and visualization of the IVC entering the RA.
4. If the IVC diameter is >2.1 cm and collapses <50% with sniff, the RA pressure is usually estimated at:
3 mmHg
5 mmHg
15 mmHg
25 mmHg
Large IVC with poor collapse indicates elevated RA pressure, commonly estimated at 15 mmHg.
5. Intermediate IVC findings (size and collapse) generally require assigning an RA pressure of:
3 mmHg
8 mmHg
12 mmHg
20 mmHg
According to ASE guidelines, intermediate IVC findings are assigned an intermediate RA pressure, usually 8 mmHg.
6. RA pressure estimation is most important clinically for calculating:
Left ventricular ejection fraction
Right ventricular systolic pressure
Mitral valve area
Aortic valve gradient
RA pressure is added to the trans-tricuspid gradient to estimate RVSP.
7. In mechanically ventilated patients, RA pressure estimation using IVC may be inaccurate because:
Positive intrathoracic pressure alters venous return and IVC size
The tricuspid valve is not visualized
Echocardiography cannot image the IVC
IVC diameter remains fixed in all patients
Positive pressure ventilation increases IVC diameter and reduces its variability, overestimating RA pressure.
8. The “sniff test” in RA pressure estimation refers to:
Assessing IVC collapse during a quick inspiratory effort
Measuring RA area during systole
Evaluating tricuspid inflow velocity
Observing jugular venous distension
The sniff maneuver transiently decreases RA pressure, causing normal IVC collapse if RA pressure is low.
9. Which factor can falsely increase RA pressure estimation from IVC measurement?
Hypovolemia
Poor inspiratory effort
Hyperventilation
High heart rate
Inadequate inspiratory effort reduces IVC collapse, mimicking elevated RA pressure.
10. When estimating RVSP, which Doppler measurement is combined with RA pressure?
Mitral E/A ratio
Pulmonary acceleration time
Tricuspid regurgitation peak velocity
LVOT VTI
RVSP = 4 × (TR velocity)² + RA pressure.
11. Which echocardiographic parameter is most commonly used to estimate RA pressure?
Inferior vena cava (IVC) diameter and collapsibility
Right ventricular outflow tract (RVOT) velocity
Mitral inflow E/A ratio
Tricuspid annular plane systolic excursion (TAPSE)
The IVC size and its inspiratory collapse are key non-invasive indicators for RA pressure estimation.
12. An IVC diameter of 1.8 cm with >50% collapse suggests an estimated RA pressure of:
0–3 mmHg
3 mmHg
8 mmHg
15 mmHg
Small IVC with >50% inspiratory collapse generally indicates a low RA pressure around 3 mmHg.
13. Which breathing maneuver is used to assess IVC collapsibility?
Valsalva maneuver
Sniff test
Breath-holding at end-expiration
Cough maneuver
The sniff test causes a sudden drop in intrathoracic pressure, helping to assess IVC collapse.
14. A dilated IVC (>2.1 cm) with <50% collapse typically corresponds to RA pressure of:
3 mmHg
5 mmHg
15 mmHg
20 mmHg
A large IVC with poor collapse is a marker of elevated RA pressure (~15 mmHg).
15. Which clinical condition is most likely to cause persistently dilated IVC with poor collapse?
Severe aortic stenosis
Acute mitral regurgitation
Right heart failure
Hypertrophic cardiomyopathy
Right heart failure increases systemic venous pressure, causing IVC dilatation and poor collapse.
16. In mechanically ventilated patients, IVC dynamics are:
Unaffected by ventilation
Reversed compared to spontaneous breathing
Identical to normal sniff test results
Irrelevant for RA pressure estimation
Positive pressure ventilation can alter IVC size changes, making interpretation more complex.
17. RA pressure is an important variable for calculating:
Mitral valve area
Pulmonary artery systolic pressure
Ejection fraction
Aortic valve gradient
RA pressure is added to the tricuspid regurgitant gradient to estimate pulmonary artery systolic pressure.
18. When IVC diameter and collapse are intermediate, RA pressure is usually assigned as:
3 mmHg
5 mmHg
8 mmHg
15 mmHg
Intermediate IVC measurements are usually assigned a mid-range RA pressure of 8 mmHg.
19. A patient has IVC 2.5 cm with 20% collapse. Estimated RA pressure?
3 mmHg
8 mmHg
15 mmHg
20 mmHg
Large IVC with minimal collapse indicates elevated RA pressure (~15 mmHg).
20. Why is RA pressure estimation important in the context of tricuspid regurgitation assessment?
It allows accurate calculation of pulmonary artery pressures
It determines left ventricular diastolic function
It guides mitral valve replacement timing
It is only useful in pericardial disease
Adding RA pressure to the TR gradient from Doppler provides a non-invasive estimate of pulmonary artery systolic pressure.
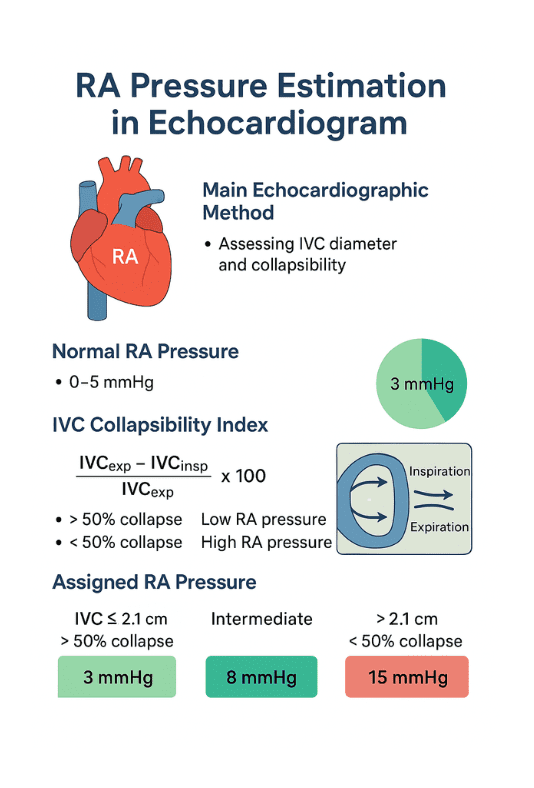
1. What is the main echocardiographic method for estimating RA pressure?
- By assessing inferior vena cava (IVC) diameter and its collapsibility during inspiration.
- Uses subcostal long-axis view.
- IVC ≤ 2.1 cm with > 50% collapse → normal RA pressure (~3 mmHg).
- IVC > 2.1 cm with < 50% collapse → high RA pressure (~15 mmHg).
- Intermediate findings → RA pressure ~8 mmHg.
2. What is the normal RA pressure range in echocardiography?
- Typically 0–5 mmHg in healthy adults.
- ASE guidelines use 3 mmHg for low, 8 mmHg for intermediate, 15 mmHg for high.
- Based on IVC size and collapsibility index.
- Values are estimates, not invasive measurements.
- Catheterization confirms actual pressure.
3. What is IVC collapsibility index?
- Formula: (IVC_exp – IVC_insp) / IVC_exp × 100.
- 50% collapse → low RA pressure.
- < 50% collapse → elevated RA pressure.
- Measured during sniff or deep inspiration.
- Reflects right atrial filling pressure changes.
4. Which factors can falsely elevate RA pressure estimation?
- Mechanical ventilation (positive pressure).
- Athletes with large compliant IVC.
- Severe tricuspid regurgitation.
- Pericardial diseases (tamponade, constriction).
- Increased intra-abdominal pressure.
5. How does mechanical ventilation affect RA pressure estimation?
- Positive pressure reduces IVC collapse.
- Can mimic high RA pressure.
- Inverse relationship with spontaneous breathing findings.
- Requires cautious interpretation.
- In such cases, invasive measurement is more reliable.
6. What RA pressure value is assigned to IVC ≤ 2.1 cm with > 50% collapse?
- 3 mmHg (low RA pressure).
- Suggests normal right-sided filling pressures.
- Often seen in healthy individuals.
- No significant right heart overload.
- Confirms adequate venous return compliance.
7. What RA pressure value is assigned to IVC > 2.1 cm with < 50% collapse?
- 15 mmHg (high RA pressure).
- Suggests right-sided congestion.
- Often seen in heart failure, pulmonary hypertension.
- Indicates elevated venous pressures.
- Requires further clinical correlation.
8. What does an intermediate IVC pattern indicate?
- IVC size and collapsibility do not fit extremes.
- Assigned 8 mmHg RA pressure.
- Reflects moderate right atrial pressure.
- May occur in early right heart dysfunction.
- Interpretation depends on clinical context.
9. How is RA pressure related to pulmonary artery systolic pressure (PASP) estimation?
- PASP = 4 × (TR velocity)² + RA pressure.
- TR velocity measured via Doppler.
- Accurate RA pressure estimation improves PASP accuracy.
- Overestimation can lead to false diagnosis of pulmonary hypertension.
- Underestimation can miss severe cases.
10. Why is invasive measurement sometimes preferred over echo estimation?
- Echocardiography is indirect and assumption-based.
- Invasive right heart catheterization measures RA pressure directly.
- Needed when clinical suspicion is high but echo is inconclusive.
- Useful in complex cardiopulmonary disease.
- Provides gold-standard hemodynamic data.
| Parameter | Criteria | Estimated RA Pressure | Clinical Notes |
|---|---|---|---|
| IVC diameter < 2.1 cm + > 50% collapse with sniff | Normal size, good collapse | 3 mmHg (range 0–5) | Suggests normal RA pressure and normal RAP waveform |
| IVC diameter > 2.1 cm + < 50% collapse | Dilated, poor collapse | 15 mmHg (range 10–20) | Suggests elevated RA pressure; check for RV dysfunction, pulmonary hypertension |
| Mixed pattern | Either small diameter + poor collapse OR large diameter + good collapse | 8 mmHg (range 5–10) | Intermediate category; consider other echo signs (hepatic vein flow, RA size) |
| Markedly dilated IVC, fixed diameter | No inspiratory collapse | 20 mmHg+ | Seen in tamponade, severe TR, constrictive pericarditis |
| IVC < 1.5 cm, collapses fully | Very compliant | 0–3 mmHg | Often seen in hypovolemia |
| Use in TR velocity–Bernoulli calculation | Add estimated RA pressure to RV–RA gradient | — | Essential for RVSP calculation |
| Alternative signs when IVC view not possible | Hepatic vein flow, RA area, right heart strain | Varies | Used when subcostal IVC imaging is suboptimal |
| Respiratory variation considerations | Assess collapse with sniff or quiet inspiration | — | Avoid deep exaggerated inspirations in patients with lung disease |


